Data on the bio-distribution of Pfizer's pseudo-vaccine shows that it doesn't enter cells, and doesn't produce any spike protein. It does, however, produce enormous damage to all organ systems. Here, we provide an answer to Facta's debunkers.
Dr. Stefano Scoglio, Ph.D.
2021 (Read in Italian)
At the current time, I am a constant target of the Facta organisation. These are the toy soldiers of the dominant narrative whose purpose is not to prove anything, but only to shout that whatever I say is false. In short, it seems that my arguments have hit the mark, and are touching on essential contradictions and inconsistencies of the dominant pseudo-scientific narrative. My arguments are therefore to be branded as fake news. This time they have it in for an article in which I explain why, according to the scientific literature, the RNA or DNA vaccine technology and RNA/DNA drug technology have not managed to solve the fundamental problem of delivery, that is, the ability to carry the genetic material into the cell. In support of my thesis, I have brought abundant scientific evidence in the form of all the articles that were published on the subject for the period of 2018-2021, articles which unequivocally show that there are 5 fundamental obstacles to the entry of synthetic RNA/DNA into the cell:
- the large abundance of extracellular ribonucleases, which break down any foreign genetic material;
- the fact that the portion that survived the attack of the aforementioned ribonucleases would then have to enter the cell through endocytosis, but often what happens is exocytosis, i.e. the cell invaginates the vaccine material, but to keep it out, not to bring it in;
- the fact, recognised by all scientists who deal with the matter, that the endosome / lysosome endo-cellular system captures, breaks up and expels more than 98% of the foreign material that enters it;
- the further existence of ribonucleases inside the cell, which would finish the work already done by the extra-cellular ribonucleases;
- finally, the most important element, i.e. the fact that this synthetic genetic material, RNA or DNA, is "intrinsically immunogenic", i.e. it is so toxic, with recognised inflammatory, autoimmune hyper-stimulation, generation of systemic oedemas and venous thrombi, as to immediately trigger the disruptive reaction of the immune system against the injected serum, thus making the action of the other aforementioned factors not even necessary.
So, how do the debunkers answer this? Listen closely:
“Scoglio cites some scientific review articles published in past years, in which the technological difficulties relating to mRNA vaccines were discussed, in order to argue that, in trying to make vaccines work, there would still be insurmountable problems: the mRNA contained in vaccines would not be capable of entering cells and, if it did, it would be immediately destroyed by specific enzymes, known as intracellular ribonucleases. We don't need to go into the details of Scoglio's arguments to know that they are wrong. We have experimental data, which tell us that the vaccine actually induces the production of spike protein in the body."
In summary, they claim that my statements are false, and to say this "there is no need to go into the detail of my arguments"! As I wrote in another article about the debunkers: that's how it is because that's how it is!
These characters are almost pitiful. In order to be able to say that my theses are false, they must also reduce my position to a minimum. Of the 5 factors indicated above, they only mention the intracellular ribonucleases, the last and least of those factors. They thereby falsify my position by reducing it to its least important topic.
The debunkers then claim:
“Regarding intracellular ribonucleases, mRNA vaccines are modified exactly like the cell's natural mRNA to prevent them from being degraded by these enzymes.”
It is true that there is research in this sense, but it is equally true that the researchers themselves state that this research is not yet satisfactory, and that the challenge of protecting genetic material not only from the sole factor that the factcheckers want to talk about, but also from the other factors I listed above, is still an open problem. I'm not going to repeat here every deliberately partial and manipulative thing that the debunkers say, but in the article you will find all the quotes that confirm what I say, from the fact that the cell constitutes a "formidable barrier" for everything that you want to introduce into it, to the fact that the endosome / lysosome system eliminates more than 98% of the material that could possibly enter.
The debunkers argue that, beyond the theoretical discussion, the fact that synthetic RNA/DNA vaccines are able to produce the proteins they are designed to produce is confirmed by experimental data, i.e. by the fact that in very few studies, have researchers concluded having found the specific proteins in the body (in the case of coronaviruses, the spike protein) that the RNA/DNA was supposed to produce.
I don't know if it's out of ignorance or out of a desire to mystify, but the factcheckers obscure the difference between the direct retrieval of these proteins in the blood and their indirect retrieval via antibodies. Perhaps it's because they don't want people to know that the post-vaccination proteins are never found directly, but only ever through antibodies.
And this is another crucial point: finding proteins directly in the body is not difficult, But why do researchers not go looking for the proteins themselves instead of the antibodies to those proteins? And if, as I maintain, antibodies are not specific, it is clear that their value as an indicator of the presence of this or that protein is null and void.
Here too, the debunkers do not enter into the merits of my statements, but, as usual, limit themselves to the argument from authority:
“These are grossly incorrect claims, at odds with the basis of immunology.”
I mean, I'm wrong because I don't accept the dominant doxa. In reality, they themselves open up the possibility of the non-specificity of antibodies:
“As the CNR researcher quoted by Scoglio says on page 12 of the document, it is true that in some cases an antibody can react with several different molecules, a phenomenon which leads, for example, to cross allergies, in which an allergy to a substance can induce also allergy to another, but this does not mean that antibodies bind indiscriminately to any antigen.”
In fact, an antibody does not necessarily react indiscriminately to any antigen, but the fact that it can react to multiple antigens should already raise the question of their fundamental specificity.
The antibodies that are tested are (almost) always limited to two: IgM and IgG, and these two antibodies must be specific for billions of viruses and bacteria. How is this possible? Are there billions of subgroups of these IgG and IgM? No, there is no subgroup. This is what happens: serum is taken from the blood of the subject to be tested, and through different procedures, for example the ELISA test, the serum containing the antibodies of the subject is brought into contact with the antigen whose specificity is to be tested. Apart from the fact that the virus has never been purified and so it is not known what is being used as an antigen, if the antibody is activated when in contact with this "antigen", then it is said to be specific for that antigen. In practice: vaccines, as we have said, are highly "immunogenic", which means that they independently stimulate the production of antibodies in the recipient. But instead of attributing the increase in antibodies to the toxicity of the vaccine, the serum of the vaccinees is taken, put in contact with the artificial spike protein (produced in a laboratory and not deriving from any natural virus), and if there is a reaction of the subject's antibody to the artificial spike protein (whose toxicity has been proven) then the vaccine is said to be effective, since it stimulated the production of antibodies against the virus. The problem is that all these tests are done without controls!
The correct way to proceed would be as follows: the patient's serum is taken and put in contact not only with the artificial antigen of the presumed virus, but also with the vaccine, with other presumed pathogens and toxins, and only if the antibody is activated exclusively with the spike protein and with no other toxins or pathogens, only then can we say that the antibody is specific. This is never done. The serum is tested exclusively with the selected antigen. In this way, it is almost guaranteed that every time the antibody is tested against an antigen it is activated against that antigen. In short, if you want to prove that you have antibodies against malaria, test the serum only with the malaria antigen; when you want to demonstrate that you have specific antibodies for E.Coli, test the patient's serum only with E.Coli; and so on. Ultimately, it is a scam which, by sequentially testing a universal antibody each time with a different antigen and only with that antigen, leads us to believe that there are specific antibodies for each different toxin or pathogenic material; whereas the antibody reacts to all pathogenic factors precisely because it is universal and generic. Much pseudo-science and chemotoxic medicine is based on this scam.
I realise that the questioning of the antibody method touches a raw nerve, and that even many critics of the SARS-Cov2 virus thesis don't feel like going so deeply into the critique of virology. But someone needs to do it, even at the cost of accusations and defamations coming from the mainstream.
And so, I now come to the definitive proof that what I say about the impossibility of the gene serums entering the cell is true. That is, the Japanese government study on the bio-distribution of the Pfizer vaccine.
This is a study carried out by the Japanese Government and which Pfizer has done everything to keep secret, but which has been made public thanks to a FOIA.
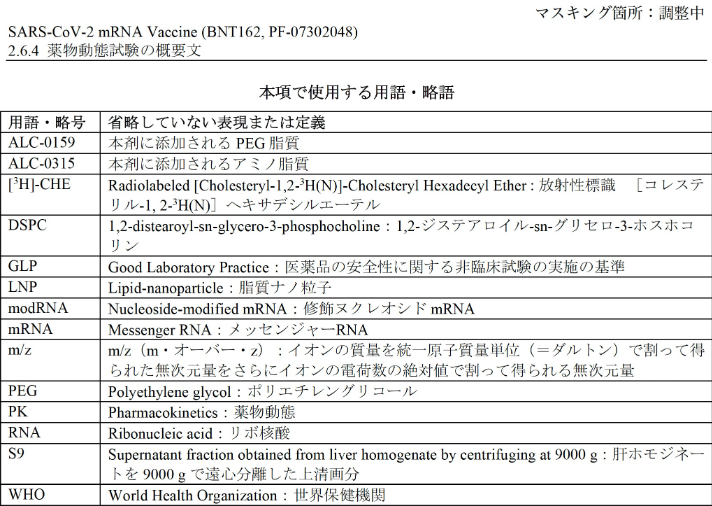
The article is in Japanese, and attached to this article you will find the translation made by the undersigned. I don't know Japanese, and I translated through Google Translate, which obviously translated awkwardly, but I managed to reconstruct a sensible and substantially correct interpretation of the article. This is also thanks to the fact that the tables with the numerical data, and the relative legends, are in English (left in the original English in the translation). The test, which was carried out in collaboration with Pfizer itself, took place as follows.
The researchers evaluated the bio-distribution of lipids that encapsulate the mRNA in the body, through a double detection system: encoding the mRNA for the fluorescent enzyme luciferase, or making the lipids radioactive. The research focused on the lipids ALC-0315 (aminolipid) and ALC-0159 (PEG lipids), while ignoring the finding of nucleic acids and metabolites produced by the metabolites of the spike protein that should have been produced with the entry of the
vaccine material into the cell. Actually, it would have been interesting to verify these last two factors as well, but obviously, with the researchers being linked to Pfizer, they had to assume, at least a priori, that the spike protein and nucleic acids derived from the endocellular decomposition of the mRNA were formed, even if the conclusions of the study, as we shall see, demonstrate the exact opposite. In fact, the official narrative on the functioning of these genetic pseudo-vaccines, which is taken for granted even by "alternative" researchers, is that the vaccine material enters the cell thanks to the lipids that act as transporters via the mechanism of endocytosis; so that the mRNA reaches the cellular ribosomes to instruct them to generate the spike protein of the presumed virus. In this model, the mRNA, once its work is done, is degraded by the endocellular enzymes into nucleic acids (it is not clear why these endocellular enzymes, the ribonucleases but also the endosome / lysosome system should degrade the mRNA after and not before it has accomplished his deed). The same thing would happen to the lipids that would have transported the mRNA into the cell, they would also be degraded into their lipid metabolites, such as chylomicrons in the case of cholesterol. In this sense, if the model proposed by Pfizer, Moderna and Astra Zeneca works, the encapsulating lipids and amines, ALC-0315 and ALC-0159 in the case of Pfizer, should in turn be degraded, through proteolysis as regards the amines and through lipolysis for lipids, and therefore they should not be found in their original form in the body of the vaccinated. But this is exactly what Japanese researchers found!
Since the translation of the article has been attached, I will limit myself to reporting the main points. Let's take this first result reported in the study:
“In our biodistribution assay, luciferase RNA-encapsulated LNP was administered intramuscularly to BALB/c mice. Consequently, luciferase expression was observed at the site of administration and the level of expression was lower than that in the liver. The administration site expression of luciferase was observed from 6 hours after administration and disappeared 9 days after administration. Expression in the liver was also observed 6 hours after dosing and disappeared within 48 hours after dosing.”The fact that the luciferase-containing material is found immediately in the liver and much less at the injection site immediately demonstrates that the vaccine does not work as expected. In fact, according to the official narrative, the vaccine material, once injected, should be rapidly absorbed by the dendritic cells, where it should precisely stimulate the production of spike protein. Instead, here we see that the injected material almost instantaneously passes into the liver, as evidenced by the fact that it is found both in the injection site and in the liver after the same 6 hours. The very fact that after 9 days the unchanged drug is found in quantity at the injection site is further proof that it does not enter the cells, where it would be rapidly metabolised, but rather remains in the tissues in an unaltered form.
As can be seen in Table 1 (from the translated article), the vaccine material almost immediately passes into the liver in large quantities, as much as 60% of the total in the case of ALC-0315 and 20% in the case of ALC-0159. From the liver, as we will see, the material circulates to all the organs, where it is deposited, except for the portion which is excreted.
That the material circulating in the injection site (& as we will see, in all the organs) is in fact the unmodified drug, which therefore never entered the cells, is also proven by tissue analysis of the of post-vaccinated animals:
“The proportion of unchanged drug after inoculation was measured to see which of ALC-0315 and ALC-0159 was also metabolically stable in animal species and test systems, with a final percentage of the unchanged drug that was greater than 82%.”This data, in itself, puts an end to the illusion that the genetic material enters the cells and triggers the production of spike protein. The 82% refers to the total material contained in the tissues, not to the total material injected, because the analysis of the vaccine material content in urine and faeces confirms that about 50% of the injected material is excreted:
“Concentrations of ALC-0315 and ALC-0159 in urine and faeces collected over time were measured. Neither ALC-0315 nor unchanged ALC-0159 were detected in urine, but were found in faeces, where unchanged forms of ALC-0315 and ALC-0159 were detected, at a rate of approximately 1% per dose, respectively, and constituted about 50% of the total.”Thus, approximately 50% of the injection's total content is excreted unchanged from the form in which it was injected. Of the remaining 50% that remained in the body, 82% remained unchanged, in the form in which it was injected, while the remaining 18% was metabolized, not at the intracellular level but through enzymatic mechanisms described in figures 3 4 If the metabolites were the product of intracellular degradation, they would already be formed in the bloodstream. Instead, they are formed through a progressive series of enzymatic degradation mechanisms in the blood and liver. This confirms that even the remaining 18% of the non-excreted material, equal to 9% of the total injected content, is degraded, perhaps ending up in the urine, outside of the cells. From this it emerges that 91% (50% + 82% of 50%) of the inoculated material is either excreted or deposited in organs and tissues, while the remaining 9% is enzymatically degraded in the blood and liver, before it can enter any cells.
What is strongly relevant is the important presence of the unaltered vaccine material, with its infinitesimal nanometric particles, in all organs, with a massive presence in organs such as the liver, spleen, adrenal glands and ovaries, as demonstrated by the attached Tables 2.6.5.5B:
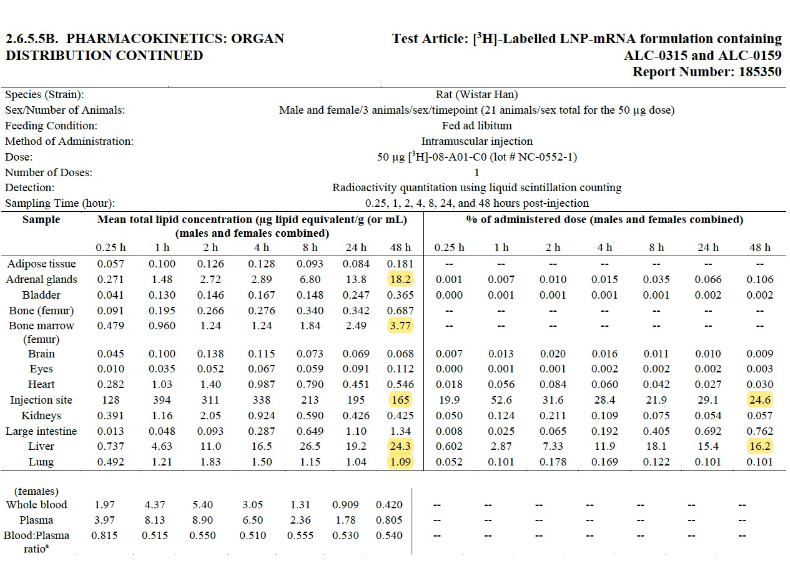
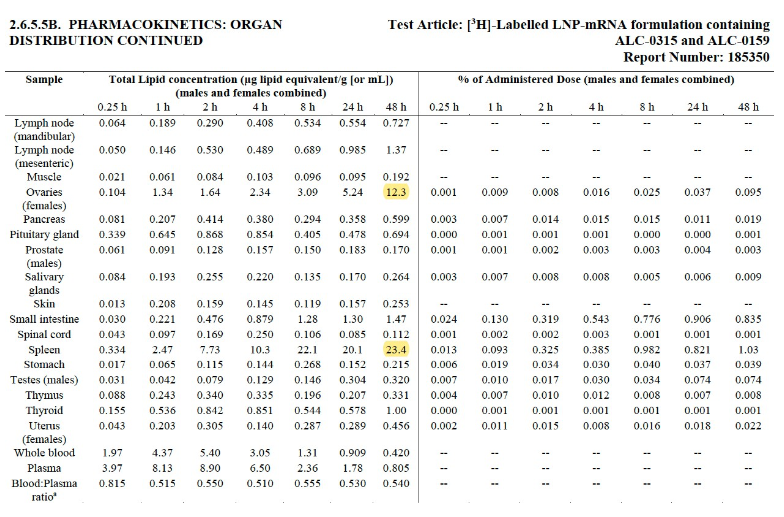
As can be seen from these tables, the mRNA encapsulating lipids ALC-0315 and ALC-0159 are dispersed, in their original formulation in unaltered nanoparticles, in all organs. If the lipids and mRNA, encoded with a radioactive or fluorescent marker (luciferase), had entered the cells to produce the spike protein, they would have been metabolised, degraded into their metabolites, and therefore it would not have been possible to find them unchanged in the organs, as actually occurred. This confirms my statement that the intrinsic toxicity of this material, the so-called immunogenicity of the pseudo-vaccine, triggers such an immune reaction that the vaccine material explodes into its innumerable constituent nano-particles, which spread and deposit in all organs of the body, in particular, as evidenced by the yellow underlining, in the liver, spleen, adrenal glands and ovaries.
However, the main place of storage remains the injection site, where the vaccine material remained for a good 9 days before being excreted via the faeces (directly) and the urine (metabolised) by about 50%, with the rest (unaltered) then ending up in the organs. In fact, if one looks at the progression of the concentrations, one sees that as the concentration of lipids at the injection site decreases, passing from 394 after 1 hour to 164 after 48 hours, the concentrations of the same lipids progressively increase in all the organs. For example, it goes from 4.63 after one hour in the liver to 24.3 after 48 hours. This further confirms that the vaccine material, once inoculated, remains for 9 days at the injection site, and without being absorbed by the dendritic cells, its concentration progressively decreases as it transfers its share of material to all of the organs via the bloodstream.
There is one last point related to entry into the cells. In the Japanese study, in Figure 3, we talk about the metabolisation of the two lipid compounds also in the hepatocytes, which are the liver cells, and this would suggest that the vaccine material then enters the hepatocytes, and would therefore have some chance of reaching the ribosomes. But if you look closely, you will see that the authors speak of monkey and human hepatocytes, i.e. the tissues used for in vitro analysis, not of mice and rats, the only animals on which bio-distribution was evaluated. Therefore, not only is this data not relevant for the effective metabolism of the serum, but it must also be said that in vitro cells are much weaker, they no longer constitute that "formidable barrier"1 of live cells which are part of a living organism, and therefore with in vitro cells something can be done.
I conclude this article with an emphasis on how the mRNA and these highly immunogenic synthetic lipids, which are deposited in the organs, are highly toxic and generate significant damage in the body. It was already clear that the fate of the mRNA-encapsulating LNPs was to deposit themselves in the organs, from where they are very difficult to clear:
“...large cationic LNPs fail to extravasate from the capillaries found in the lungs and cannot be filtered from the bloodstream by the kidney. This can lead to the accumulation of delivery materials in the liver, lungs, or other organs”2And once in the organs, in all organs as we have seen, even if in different concentrations, these LNP particles manifest their iatrogenic character:
“...some mRNA-based vaccine platforms induce potent type I interferon responses, which have been associated not only with inflammation but also potentially with autoimmunity…Another potential safety issue could derive from the presence of extracellular RNA during mRNA vaccination. Extracellular naked RNA has been shown to increase the permeability of tightly packed endothelial cells and may thus contribute to oedema. Another study showed that extracellular RNA promoted blood coagulation and pathological thrombus formation."3Inflammation, autoimmunity, systemic oedema formation, pathogenic thrombus formation. I'd say this would be enough by itself!
But as the quote above already indicates, synthetic mRNA itself is a source of toxicity:
“...mRNA molecules are themselves a PAMP when delivered to cells exogenously....However, the intrinsic nature of these PAMPs may make it difficult to modulate the inflammatory profile or reactogenicity of...vaccines.”4That is, the level of toxicity of the mRNA makes it difficult to control the inflammation generated and the reactivity, or stimulation of an uncontrolled response by the immune system, which, as we have seen, is the main reason for the vaccine's ineffectiveness and its dispersion in all organs in the form of nanoparticles. Let's not forget that in the same trial of the Pfizer Phase I/II vaccine, extensive damage was found in the guinea pigs:
“Related adverse events were reported by 25%...in the 10 μg group, [and by] 50% in the 30 μg and 100 μg groups.”5And the dosage chosen by Pfizer for the human anti-Covid vaccine was that of 30 μg. Further, it has long been known that nucleoside analogues, i.e. synthetic mRNAs, “...demonstrated unexpected mitochondrial toxicity.”6
In this regard, the authors cite several articles”7, one of which, even dated 1995, where it was found that an artificial analogue nucleoside, developed to treat chronic hepatitis B, actually caused severe liver failure (hepatic failure) and lactic acidosis.8 This is what a recent article on the subject concludes:
“The flip side of the possibly beneficial adjuvant inflammation, however, is potential toxicity of the mRNA vaccines...Such toxicities...Such toxicities… have been seen with drugs that contain unnatural modified nucleosides. The clinical adverse effects have included myopathy (caused by mitochondrial toxicity), lactic acidosis, pancreatitis, lipodystrophy, liver steatosis, and nerve damage; certain ones have been fatal.”9
Pretty impressive as side effects go, including some fatal ones, and especially those that involve all the physiological domains, from muscles (myopathies) to the pancreas, to the liver to the nervous system all the way to lipid and glucose metabolism (lipodystrophy).
In short, we could go on for pages with data like this, because it is clear that all scientific articles, even the most recent ones, underline the broad-spectrum toxicity of both synthetic mRNA and LNP lipid compounds. Given these scientifically proven bases, the inability of the serum to enter the cell and produce the spike protein, together with its broad and high level of toxicity, that marketing authorisations should have been granted, and green passes and vaccination mandates imposed, is a crime that cries out for vengeance.
***
1 Wadhwa A. et al., Opportunities and Challenges in the Delivery of mRNA-Based Vaccines,
Pharmaceutics 2020, 12, 102.
2 Kowalski PS et al., Delivering the Messenger: Advances in Technologies for Therapeutic mRNA Delivery, Molecular Therapy Vol. 27 No 4 April 2019, p.5.
3 Pardi N. et al., mRNA vaccines – a new era in vaccinology, Nature Reviews/ Drug Discovery, Vol 17, April 2018, pp. 261-279, p. 275.
4 Pardi N. et al., mRNA vaccines – a new era in vaccinology, Nature Reviews/ Drug Discovery, Vol 17, April 2018, pp. 261-279, p. 262, p. 268. 5 Mulligan MJ et al., PhaseI/PhaseII study of Covid-19 RNA vaccine BNT162b1 in adults, Nature, Vol 568, 22 Oct 2020, pp. 589-93.
6 Sahin U. et al., mRNA-based therapeutics - developing a new class of drugs, NATURE REVIEWS | DRUG DISCOVERY VOLUME 13 | OCTOBER 2014 | 759.
7 Lewis, W. et al. Fialuridine and its metabolites inhibit DNA polymerase γ at sites of multiple adjacent analog incorporation, decrease mtDNA abundance, and cause mitochondrial structural defects in cultured hepatoblasts, Proc. Nat.Acad. Sci. USA, 93, 3592–3597 (1996).
8 McKenzie R. et al.,Hepatic failure and lactic acidosis due to fialuridine (FIAU), an investigational nucleoside analogue for chronic hepatitis B. N. Engl. J. Med. 333, 1099–1105 (1995). The Japanese study would seem to disprove this liver toxicity, since the researchers conclude that the mRNA deposited in the liver did not cause liver toxicity. But the parameters of the toxicity test used are not declared, so this conclusion has no value.
9 Liu Margaret A., A Comparison of Plasmid DNA and mRNA as Vaccine Technologies, Vaccines 2019, 7, 37, p.8; che cita: Feng J.Y. et al, Insights into the Molecular Mechanism of Mitochondrial Toxicity by AIDS Drugs. J. Biol. Chem. 2001, 276, 23832–23837; Moyle, G. Toxicity of antiretroviral nucleoside and nucleotide analogues: Is mitochondrial toxicity the only mechanism? Drug Saf. 2000, 23, 467–481; Johnson A.A. et al., Toxicity of Antiviral Nucleoside Analogs and the Human Mitochondrial DNA Polymerase. J. Biol. Chem. 2001, 276, 40847–40857.
Source: https://www.byoblu.com/wp-content/uploads/2021/10/Lo-studio-giapponese-sulla-bio-distribuzione-del-vaccino-Pfizer.pdf
Translation: David Montoute
Nenhum comentário:
Postar um comentário